Coronary artery disease caused by plaque accumulation remains a leading health challenge globally, and the condition becomes particularly difficult to treat when calcium deposits harden inside these vital blood vessels. The traditional approach to managing such blockages combines lifestyle modifications, pharmaceutical therapy, and when necessary, surgical or minimally invasive procedures aimed at restoring normal blood flow to the heart muscle. However, severely calcified arteries present unique technical obstacles that have long frustrated cardiologists seeking optimal outcomes for their patients.
Plaque buildup inside coronary arteries develops gradually as a combination of fat, cholesterol, calcium deposits, cellular debris, and fibrin accumulate along vessel walls. Over time, this material narrows the passages through which oxygen-rich blood flows to the heart, progressively restricting circulation. When left unchecked, this narrowing or complete blockage prevents adequate blood supply from reaching heart tissue, substantially elevating the risk of myocardial infarction, heart failure, and cerebrovascular events. The severity of this threat depends on how much the vessel diameter has diminished and how critical the affected artery is to overall cardiac function.
Conventional interventional cardiology procedures such as percutaneous coronary intervention, coronary artery bypass grafting, and balloon angioplasty have proven effective for many patients. In standard cases involving soft plaque, interventionalists deploy a balloon catheter to compress the blockage, creating sufficient space within the artery for blood to flow freely again. A metallic stent is then positioned to maintain this newly opened passage and prevent the vessel from re-narrowing. Yet this straightforward approach encounters significant limitations when confronted with severely calcified lesions, as Datuk Dr Tamil Selvan Muthusamy, a consultant cardiologist, explains. The calcium hardens into such rigid deposits that conventional balloon pressure cannot adequately fracture the material, making device delivery and stent expansion problematic and often resulting in suboptimal immediate and long-term clinical results.
To address heavily calcified coronary disease, specialists have turned to more sophisticated techniques including rotational atherectomy, high-pressure balloon angioplasty, and intravascular lithotripsy. The latter represents a relatively recent innovation in which externally generated ultrasonic pressure waves are delivered through a specialized catheter to shatter calcium deposits within blood vessels. Although this technology marks a genuine advancement in treating calcification-laden arteries, intravascular lithotripsy carries inherent limitations. The number of ultrasound pulses available remains restricted—earlier devices offered only eight pulses while newer versions provide twelve—meaning clinicians must strategically deploy these limited cycles to fragment calcium deposits throughout the entire blockage.
Additional constraints affecting standard intravascular lithotripsy include device design challenges and anatomical variability. The catheter apparatus is relatively bulky, creating insertion difficulties when blockages are extensive and the remaining patent lumen becomes very narrow. Furthermore, the fixed balloon diameter cannot accommodate vessels that taper or dilate along their length. A vessel might measure 3.5 to 4 millimetres at its proximal end but narrow to 2 to 3 millimetres distally, yet the clinician must select a single balloon size. This mismatch between rigid device dimensions and natural vascular anatomy often necessitates supplementary techniques and compromises procedural efficiency.
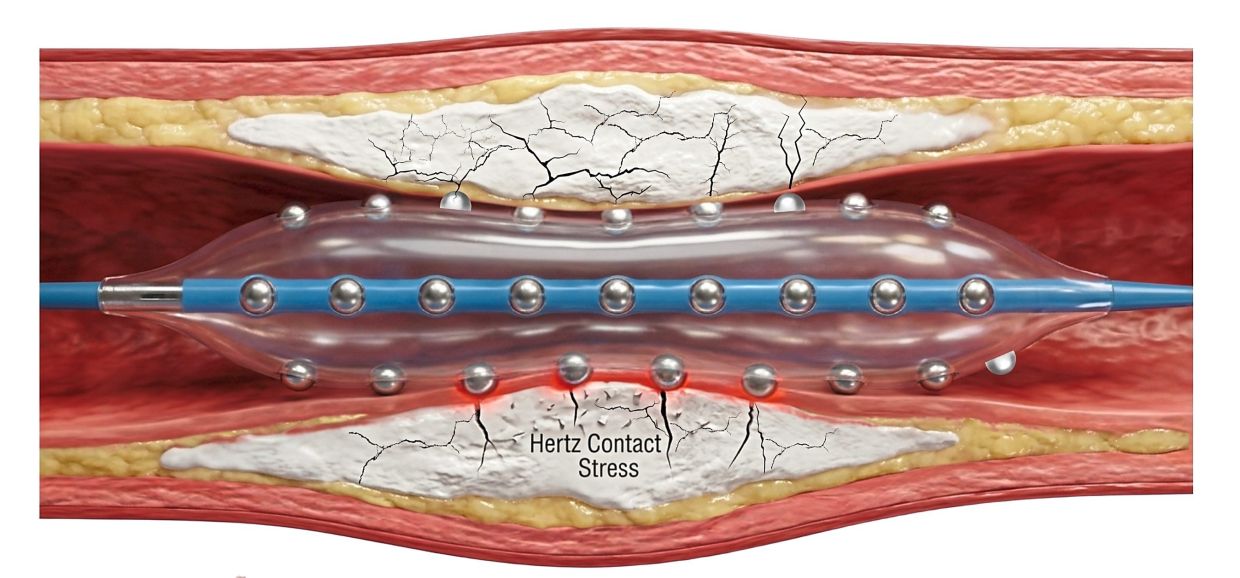
Recognizing these constraints, Malaysian cardiologists under Dr Tamil Selvan's leadership initiated a clinical investigation during 2025 into a revolutionary advancement called the Hertz Contact-Intravascular Lithotripsy System. This novel device represents a fundamental departure from energy-dependent lithotripsy by employing a mechanical approach rather than relying on external ultrasonic generators. The catheter incorporates a balloon embedded with tiny stainless steel hemispheres that, when pressed against hardened plaque, create focal pressure amplification sufficient to fracture dense calcium deposits. This mechanical principle achieves the calcium-breaking objective without requiring an external energy source, while simultaneously generating deep, wide fissures in the plaque that permit proper arterial expansion without thermal or acoustic injury to surrounding tissue structures.
The mechanical design innovation translates into practical advantages for interventionalists managing complex calcified lesions. Dr Tamil Selvan emphasizes that the integrated hemispheric structure multiplies applied pressure, transmitting force beyond the vessel wall in controlled fashion. Crucially, the enhanced deliverability characteristics allow the catheter to traverse the entire affected vessel with greater ease than conventional devices, substantially improving navigability through narrow passages. This improved trackability means a single balloon can address multiple vessels or lengthy blockage segments, streamlining the procedure and reducing the number of device exchanges required. For patients, improved efficiency potentially translates into shorter procedure times, lower radiation exposure from fluoroscopy, and reduced contrast medium administration.
The decision to undertake a comprehensive Malaysian-based clinical investigation stemmed from gaps in existing evidence regarding device safety and efficacy. While the technology's developer had sponsored small multi-centre studies across United States facilities, these investigations lacked the scale and rigor necessary to establish definitive safety profiles and real-world performance data. Dr Tamil Selvan and his colleagues recognized that expanding research beyond preliminary studies would generate higher-quality evidence specifically relevant to the patient populations and clinical environments in Southeast Asia. This locally-driven research initiative addresses a critical need in cardiac care by systematically evaluating an innovative technology that may substantially improve outcomes for patients with one of the most challenging forms of coronary artery disease.
The significance of this research extends beyond technical innovation in device design. Successfully validating the Hertz Contact-Intravascular Lithotripsy System would provide Malaysian and regional cardiologists with a powerful tool for managing complex calcified coronary lesions that currently offer limited treatment options and frequently produce unsatisfactory results. For patients with extensive coronary calcification, whose conditions may previously have required bypass surgery with its attendant operative risks and recovery demands, an effective minimally invasive alternative could transform treatment paradigms. Furthermore, the accumulating evidence of treatment success would likely influence purchasing decisions by Malaysian hospitals and clinics, ultimately improving access to advanced interventional cardiology techniques throughout the region.

